GLP-1 Patches: Why Do GLP-1 Patches Fail Under the 500 Dalton Rule?
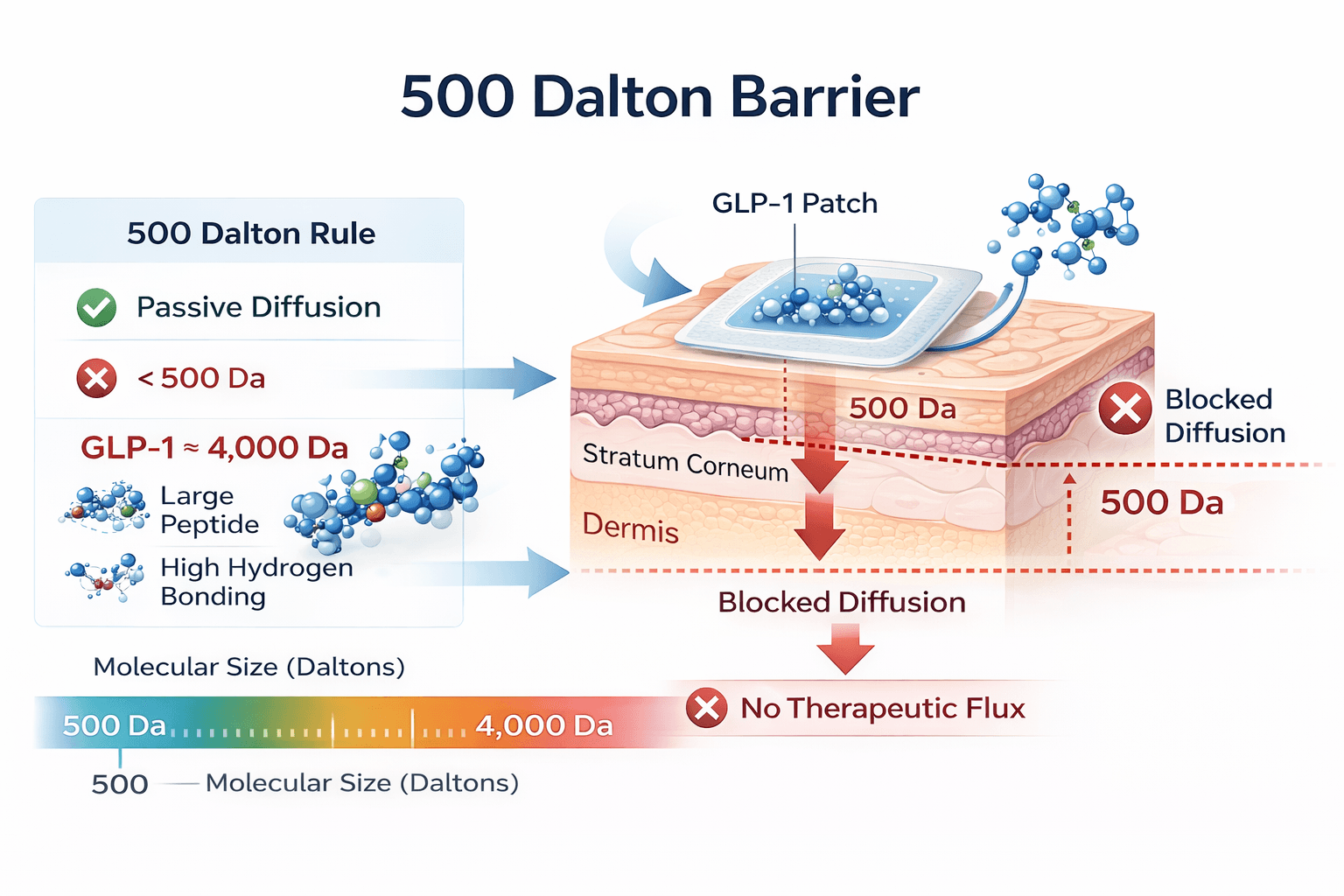
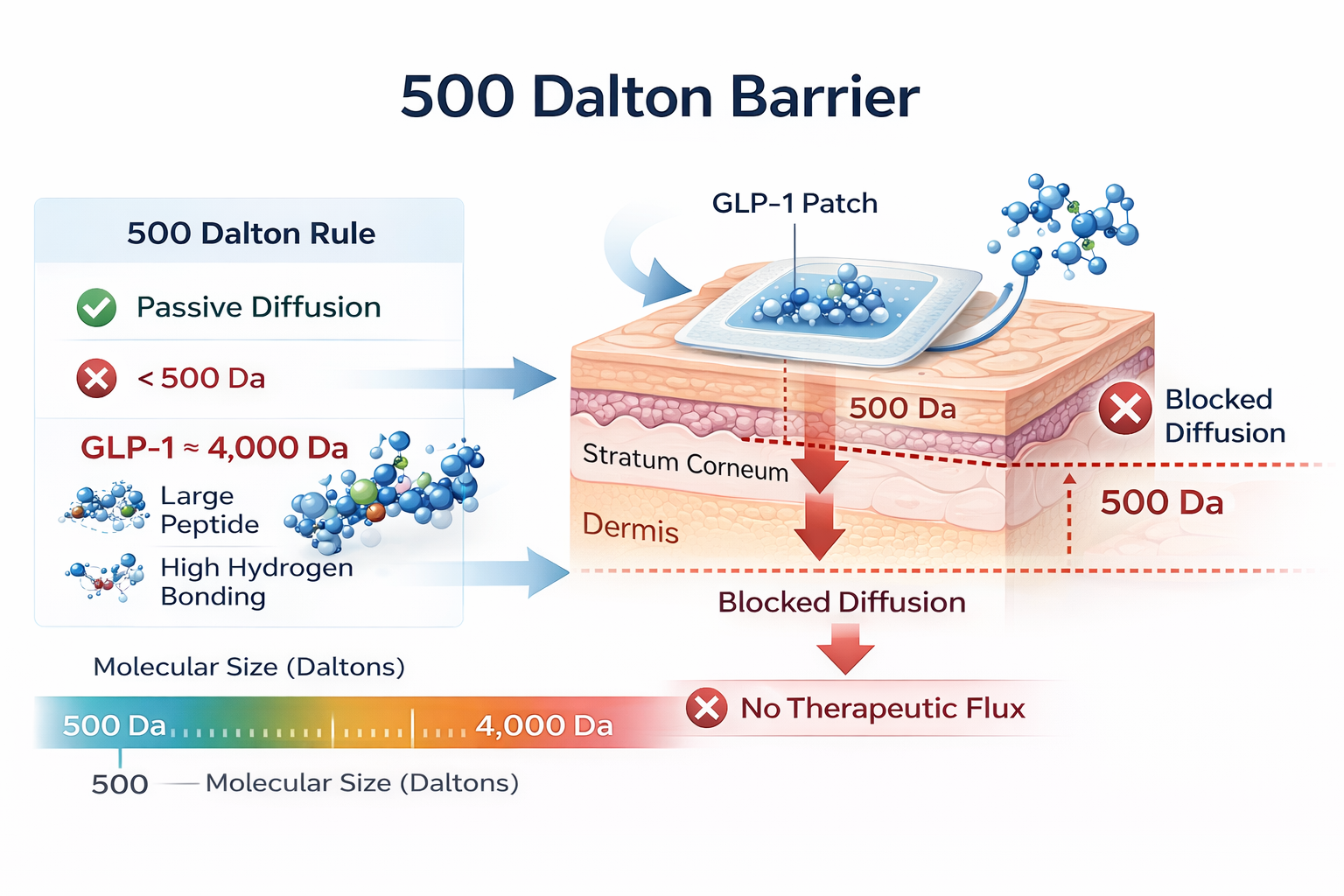
GLP-1 patches fail because GLP-1 receptor agonists are beyond the physicochemical criteria necessary for passive diffusion across the skin. The 500 Dalton rule shows that compounds larger than 500 Da are less likely to diffuse through the intact stratum corneum. Since GLP-1 is a compound of about 4,000 Daltons with high hydrogen bonding, it is not possible to achieve a therapeutically significant transdermal flux rate based on diffusion principles [1].
Understanding these delivery limitations is essential for patients and clinicians evaluating treatment claims. At EmbraceRx, we emphasize therapies supported by regulatory approval, validated pharmacokinetic data, and established clinical outcomes. Treatment decisions are grounded in evidence-based medicine rather than unverified delivery systems lacking demonstrated systemic absorption.
Why Does Skin Barrier Structure Block Peptide Diffusion?
The stratum corneum blocks peptide diffusion because it is a lipoprotein complex with high resistance to hydrophilic macromolecules. Transdermal transport is a function of molecular size, lipid solubility, and partitioning. Polar peptides are large molecules with permeability coefficients and diffusion rates that are very low and steady-state fluxes that are too low for systemic pharmacologic effects in intact skin [2].
Transdermal transport can be expressed according to Fick’s first law of diffusion:
J = (D × K × ΔC) / h
Where:
- J = steady-state flux
- D = diffusion coefficient
- K = partition coefficient (lipid/water)
- ΔC = concentration gradient
- h = membrane thickness
GLP-1 receptor agonists demonstrate:
Low lipid partition coefficients (poor K)
Large molecular radius (low D)
Extensive polarity and hydrogen bonding
The stratum corneum is a layer of corneocytes in a ceramide-rich lipid bilayer, which is a hydrophobic barrier that optimizes transepidermal water loss and prevents the entry of macromolecules. Consequently, GLP-1 peptides have very low permeability coefficients (Kp) for passive diffusion. Without mechanical or energy-assisted enhancement technologies, adhesive GLP-1 patches would not be expected to provide measurable systemic exposure.
Why Are Peptides Inherently Unsuitable for Passive Transdermal Delivery?
Peptides are unsuitable for passive transdermal delivery because of their high molecular weight, high hydrogen bonding, and low lipid partition coefficients. It has been observed in reviews of peptide and protein drug delivery that macromolecules need microneedles, iontophoresis, or other active enhancement systems to overcome the resistance of the stratum corneum. Passive adhesive patches cannot overcome these biophysical limitations [3].
The major barriers to delivery are
Low lipid solubility
Large molecular radius
Rapid enzymatic degradation
Limited dermal diffusion capacity
These factors combined result in the permeability coefficients being reduced to negligible values. As a result, the absorption of systemic peptides is scientifically impossible without active enhancement.
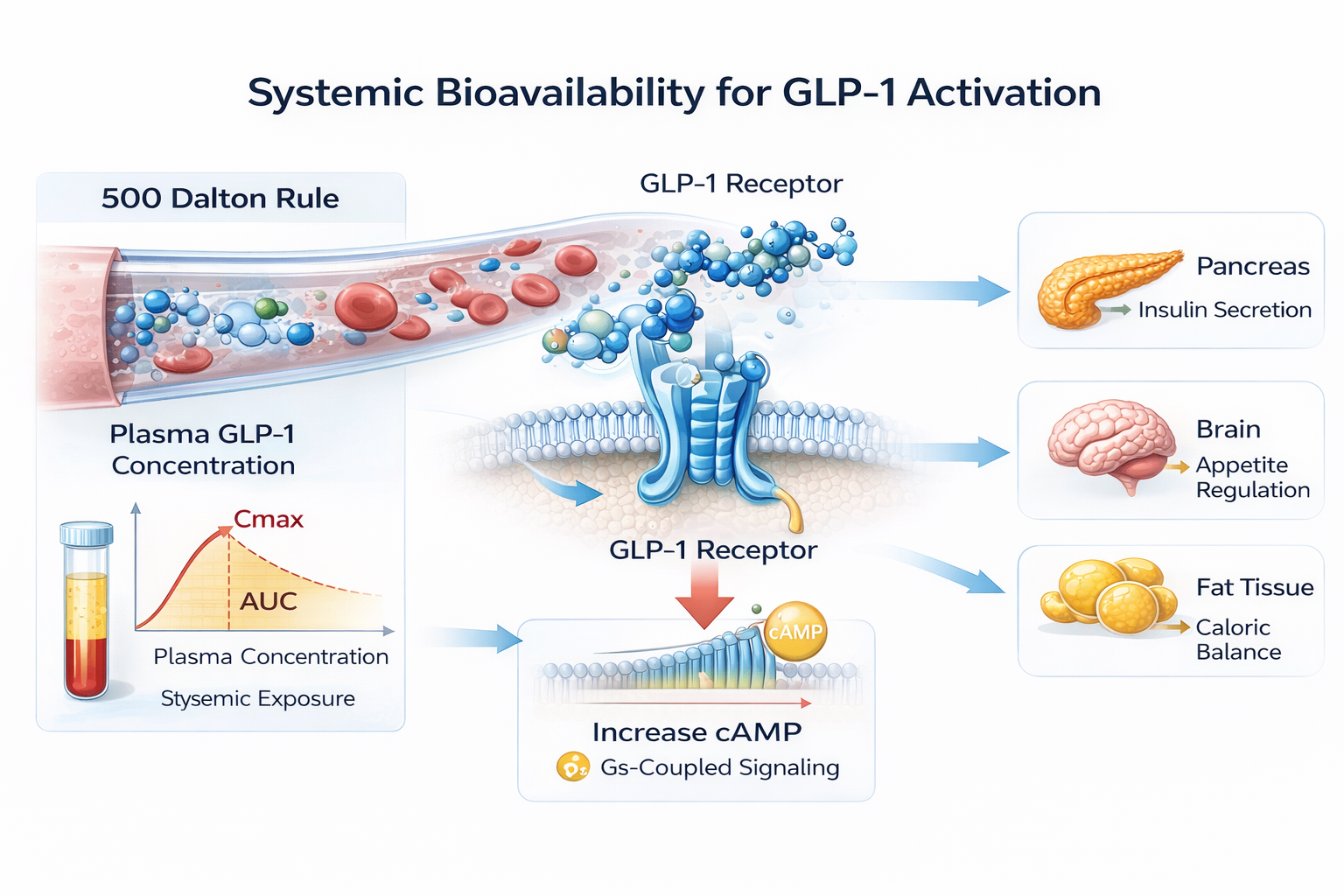
Why Does GLP-1 Receptor Activation Require Systemic Bioavailability?
Systemic exposure is a requirement for GLP-1 receptor activation to trigger Gs-coupled signaling and increase intracellular cAMP. Receptor-mediated pharmacologic effects require quantifiable plasma concentrations that can modulate pancreatic, adipose, and neural targets. The lack of pharmacokinetic parameters, such as Cmax and AUC, makes it impossible to predict receptor-mediated biological responses [4].
In addition, GLP-1 receptor signaling has dose-dependent pharmacodynamic properties, in which receptor activation, kinase activation, and metabolic responses are directly proportional to the concentration of the circulating peptide and the duration of systemic exposure. Subtherapeutic concentrations cannot provide adequate receptor occupancy thresholds to trigger sustained insulinotropic and anorectic signaling responses.
Why Do Approved GLP-1 Analogs Use Injection or Specialized Oral Delivery?
Approved GLP-1 analogs are delivered via injection or specialized oral delivery systems, since molecular engineering increases half-life but does not improve membrane permeability. Albumin binding and proteolytic resistance are improved by structural modifications such as fatty-acid acylation, which allow for extended systemic exposure. However, these modifications do not allow for passive transdermal transport across intact skin barriers [5].
Approved delivery methods include:
Subcutaneous administration
Albumin-binding prolongation
Enzyme resistance modification
Oral absorption enhancers
These delivery methods clearly show that pharmaceutical development is centered on systemic pharmacokinetics rather than transdermal transport. Development strategies have always emphasized controlled bioavailability platforms designed to deliver consistent plasma levels, supporting the notion that passive dermal diffusion is not a viable option for GLP-1 analogs.
Why Is There No Regulatory Approval for GLP-1 Patches?
There is no regulatory approval for GLP-1 patches because no transdermal formulation has been proven to have established safety, pharmacokinetics, and efficacy in clinical studies. This is because, according to regulatory guidelines, approved GLP-1 products are only injectable and oral forms that have been proven in clinical studies. Passive adhesive patches do not have documented proof of systemic absorption [6].
For regulatory approval, a thorough assessment of dose consistency, quality manufacturing standards, adverse events, and exposure-response relationships must be established through a series of clinical studies. Without human pharmacokinetic information that shows consistent plasma levels and established bioavailability, there is no way a GLP-1 patch can be approved based on established criteria for quality, safety, and performance [6].
Mechanistic Conclusion: Why GLP-1 Patches Do Not Work
GLP-1 receptor agonists are large, hydrophilic peptides with molecular weights close to 4 kDa and high hydrogen bonding capacity, making their skin permeability coefficients very low. Based on well-established diffusion principles and the 500 Dalton rule, it is clear that such peptides cannot provide a therapeutically relevant steady-state flux across the intact stratum corneum without barrier disruption or active transport technology.
Furthermore, to activate the systemic GLP-1 receptor, there has to be a measurable plasma concentration to confirm receptor activation and maintain intracellular cAMP signaling. This is presently possible with current formulations via subcutaneous injection or optimized oral absorption technology. There are no pharmacokinetic data available for passive adhesive patches to confirm bioavailability or dose-dependent systemic effects.
Evidence-Based Care at EmbraceRx
Patients are being increasingly exposed to unverified claims of GLP-1 patches that have not been pharmacokinetically validated or approved by any agency or have demonstrated any systemic absorption. Such unverified products have created ambiguity in their efficacy, quality, and safety in the management of metabolic diseases.
At EmbraceRx, GLP-1 therapy is administered through licensed medical professionals using medications that have been approved clinically for their safety and pharmacokinetics. For more information about clinically supported GLP-1 therapy options, you may contact our care team.
FAQs
Are peer-reviewed pharmacokinetic studies available to support the use of GLP-1 patches?
There are no peer-reviewed pharmacokinetic studies available in the literature to support the systemic absorption of GLP-1 peptides using passive adhesive patches. No established plasma concentration levels are available to support therapeutic bioavailability following the use of commercially available GLP-1 transdermal patches.
Why can nicotine patches work, but GLP-1 patches cannot?
Nicotine is a low-molecular-weight lipophilic compound with a molecular weight of less than 500 Daltons, allowing passive diffusion across the stratum corneum. GLP-1 analogs have a molecular weight of 4,000 Daltons and are highly polar, with permeability coefficients too low to allow for transdermal absorption.
Could microneedle systems theoretically deliver GLP-1 peptides?
Theoretically, microneedle platforms could facilitate the dermal delivery of macromolecules by overcoming the stratum corneum barrier. Nonetheless, microneedle platforms involve microstructure design, dosing validation, and pharmacokinetic studies. They are completely different from passive adhesive patches that are marketed without active enhancement technology.
Are any GLP-1 patches approved by regulatory authorities?
There is no approved passive transdermal formulation of the GLP-1 receptor agonist by any regulatory authority. The approved GLP-1 drugs are only injectable, and some oral formulations that are supported by pharmacokinetic, safety, and efficacy studies.
References